
Lucy's Love Bus supports each member of a childhood cancer family in a variety of physical settings through individual and group integrative therapy offerings.
-

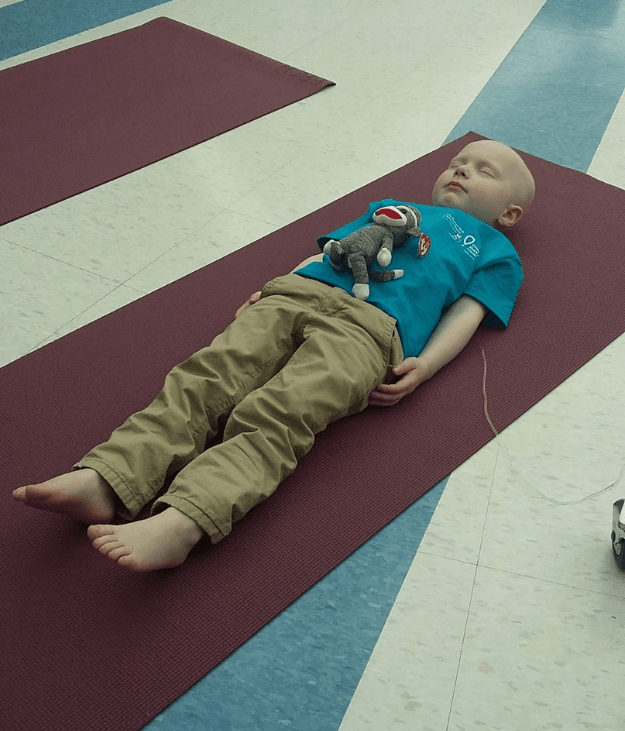
Funding for individual integrative therapies for anyone diagnosed with cancer before the age of 21, in or near their home
-
Siblings choose their own integrative therapies - either solo or with their sibling
-

Unique community-building programs for childhood cancer families, held in eastern Massachusetts or online
-
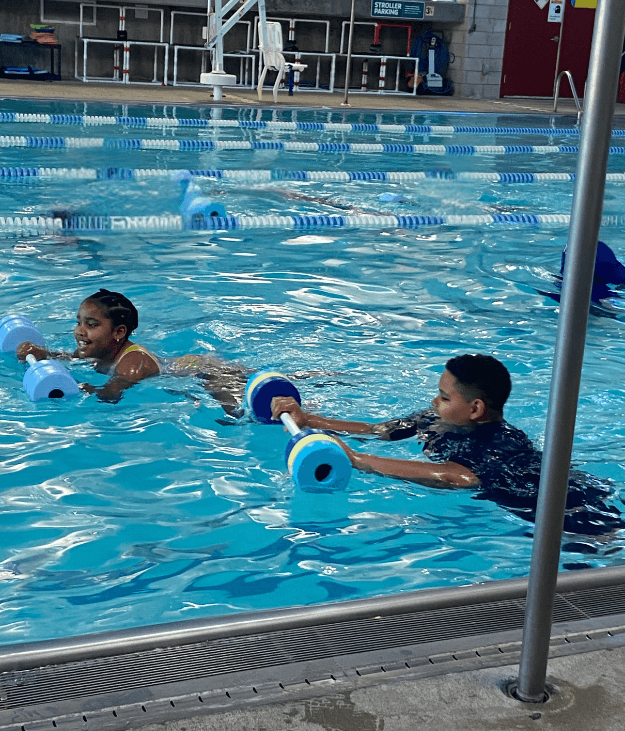
Weekly in-hospital integrative therapy sessions in four New England pediatric cancer centers
